
Efrat Shapira 1 , Ronit Ratzon 2 , Ilana Shoham-Vardi 2 , Ruslan Serjienko 2 , Moshe Mazor 1 and Asher Bashiri 1, **
Department of Obstetrics and Gynecology , Soroka University Medical Center, Ben-Gurion University of the Negev, Beer-Sheva , Israel
Department of Epidemiology and Health Services Evaluation , Faculty of Health Sciences, Soroka University Medical Center, Ben-Gurion University of the Negev, Beer-Sheva, Israel
Abstract
Objective : To compare epidemiological and obstetric characteristics, etiology and next pregnancy outcomes of women with primary vs. secondary recurrent pregnancy loss (RPL).
Study design: A retrospective cohort study, including 420 patients with two or more consecutive pregnancy losses followed by a subsequent (index) pregnancy, of whom 162 were primary RPL women and 258 were secondary RPL women. All patients were evaluated and treated in the RPL clinic at the Soroka University Medical Center.
Results : Live birth rate in the index pregnancy was not statistically different between primary and secondary RPL women (75.9 and 70.9 % , respectively). The only signifi cant difference in the etiology evaluation was in abnormal prolactin levels (14.1 % of the primary and 1.4 % of the secondary RPL group). Women with primary RPL had, at the index pregnancy, signifi cantly higher rates of preterm delivery, fetal growth restriction, and gestational diabetes mellitus. In a multivariable logistic regression analysis, primary RPL adjusted for maternal age and gravidity, was an independent risk factor for preterm delivery compared with secondary RPL [adjusted OR 2.62, CI (95 % ) 1.30 – 5.26].
Conclusions : The prognosis of the two groups was similar regarding live birth rate at the index pregnancy; however, women with primary RPL were more prone to adverse obstetric and neonatal outcomes.
Keywords: Index pregnancy; obstetric complications; pregnancy outcome; preterm delivery; primary and secondary recurrent pregnancy loss.
Introduction
A single spontaneous miscarriage is not a rare occurrence. About 15 % of clinically recognized pregnancies end in spontaneous miscarriage [17, 19, 22] . Recurrent pregnancy loss (RPL) is defi ned as two to three consecutive pregnancy losses prior to the 20 th week of gestation. The European Society of Human Reproduction and Embryology (ESHRE) defi ned RPL as three or more consecutive losses [15] . The American College of Obstetrics and Gynecology (ACOG) defi ned RPL as two or more consecutive losses [2] and the American Society for Reproductive Medicine (ASRM) defi ned RPL as two or more failed pregnancies [8] . RPL occurs in up to 5 % of women [1, 18, 20, 21] and the probable cause is found in about 50 % of patients [10, 16, 18, 22] . The rest of the cases are unexplained [10, 18] . The limited list of evidence-based factors includes chromosomal abnormalities, uterine abnormalities, endocrine disorders (thyroid disease, diabetes mellitus), antiphospholipid syndrome (APS), and acquired thrombophilias (factor V Leiden mutation) [15] . Other possible causes include other congenital thrombophilias (hyperhomocysteinemia, protein C or S defi ciencies, antithrombin mutation, prothrombin mutation) and environmental factors [10] .
RPL is defi ned as primary when all previous pregnancies ended in miscarriages and as secondary if there was at least one live birth during the woman ’ s obstetric history. The information from the current literature regarding the differences in prognosis, etiology, and the next pregnancy ’ s complications between primary and secondary RPL is inconclusive [10, 16, 18, 24] . Obstetric history seems to be an important and predictive factor of a future pregnancy ’ s outcome. Regan et al. demonstrated that primigravidas, and women with a history of only successful pregnancies, had a signifi cantly lower risk for successive miscarriage than women with previous unsuccessful pregnancies [20] . Increased maternal age and number of previous miscarriages were shown by Clifford et al. [7] to have a negative effect on subsequent pregnancy outcomes.
Supportive care in RPL was found to improve the outcome signifi cantly. However, a previous live birth conferred no advantage to the outcome of the next pregnancy [7] . Brigham et al. did not report any signifi cant difference between the two groups [5] . Alberman [1] showed that women with past live births had different epidemiologic characteristics compared to women with no successful pregnancies. The risk of another miscarriage after a series of consecutive losses (2, 3, and 4) increases signifi cantly for women with primary compared to secondary RPL.
RPL can cause frustration and distress for the woman and her partner, as well as the physician. The lack of conclusive, consistent guidelines makes it diffi cult to provide accurate consultation and management for these women, who often ask about the cause of their condition and their chances of success in the next pregnancy.
The main aim of our study was to compare medical and obstetric characteristics as well as pregnancy outcomes of women with primary vs. secondary RPL attending an RPL clinic in Soroka University Medical Center.
Materials and methods
Study population
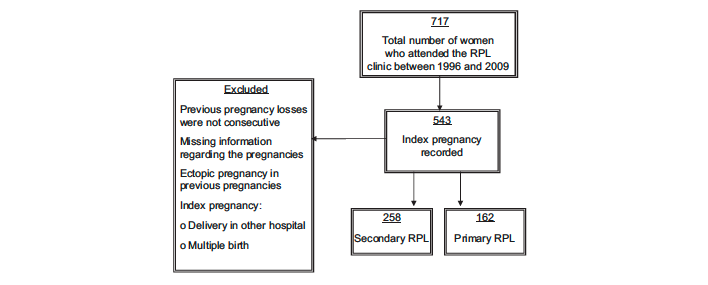
The study population included women who attended the RPL clinic Soroka University Medical Center between 1996 and 2009. Our medical center receives patients mainly from the area and its population comprises Jewish and Bedouin people, all of whom carry a universal national health insurance. The RPL clinic receives referrals for women who had recurrent miscarriages. In the clinic, women are examined and receive consultation and treatment according to the cause of RPL found after investigation. An RPL Clinic Database (Access 03) was developed by Asher Bashiri. This retrospective cohort study includes women who, upon registration at the RPL clinic, had two or more consecutive spontaneous miscarriages before 20 weeks of gestation, and following an evaluation in the clinic, had a record of a subsequent (index) pregnancy. A total of 420 women were included in this study, 39 % (168) of whom had no live birth before the index pregnancy (primary RPL). The remaining 61 % (258) had at least one live birth during their obstetric history (secondary RPL).
Exclusion criteria Missing information regarding the pregnancies, delivery in another hospital (not our medical center), multiple births at the index pregnancy, or ectopic pregnancy in previous pregnancies. A fl owchart demonstrating the inclusion of women in the study is presented in Figure 1.
Data collection
Information (demographic and clinical characteristics such as parents ’ ages and occupations, ethnicity, chronic diseases and routine medications, obstetric history, results of previous evaluations for RPL) was obtained at intake. Information about the index pregnancy was collected from medical records. Patient intake information was entered onto a spreadsheet database. In the second stage, information was abstracted from medical charts and used to verify information obtained from the patient. All the information was checked independently by two physicians, to make sure that all the pregnancies and women ’ s relevant data were recorded. In the preconception visits to the clinic, a thorough medical and obstetric history was obtained for each patient, and a physical examination was performed. Each patient was referred to a full investigation, in order to fi nd an etiology for the RPL, unless she was already pregnant. The evaluation consisted of: karyotypes of both partners; anatomic evaluation of the reproductive tract by hysteroscopy or 3-D ultrasound; hormonal evaluation by blood tests for prolactin, TSH, and fasting glucose; autoimmune disease, including tests for lupus anticoagulant activity [dilute Russell viper venom test and partial thromboplastin timelupus anticoagulant (PTT-LA), confi rmed by a hexagonal phase phospholipid test], and IgG and IgM anticardiolipin. Thrombophilic workup included: testing for protein C activity; protein S activity; antithrombin activity; activated protein C resistance; factor V Leiden mutation; and factor II mutation. Test results were added to the patient charts.
Following the investigation, patients were accepted to the RPL clinic at the beginning of the index pregnancy. At the fi rst visit, in order to defi ne pregnancy location as well as fetal viability, a transvaginal ultrasound examination was performed using transducers 7 – 4 MHz. Thereafter, they were seen in the same RPL clinic on a regular basis every 3 – 4 weeks until delivery, in addition to the ambulatory routine follow-up.
Pregnancy was ascertained by ultrasound examination or a histopathologic report. Pregnancy loss was defi ned as any spontaneous miscarriage occurring at or before 20 weeks of gestation, or with a fetal weight ≤ 500 g, including intrauterine fetal demise. Ectopic pregnancies and termination of pregnancy were counted in each patient ’ s total pregnancies, but were not considered to be spontaneous pregnancy losses. The miscarriages were divided into three groups: pre-clinical loss (demise ≤ 6 weeks of gestation), embryonic loss (demise ≥ 6 weeks but < 10 weeks of gestation), and fetal loss (demise at ≥ 10 weeks but < 20 weeks of gestation). Ante-partum death was defi ned as pregnancy loss occurring after 20 weeks of gestation until birth. Post-partum death was defi ned as infant death occurring from birth until day 7 after birth. Small for gestational age (SGA) and large for gestational age (LGA) were defi ned according to birth weight standards in the live-born population in Israel [9] . Low birth weight (LBW) is defi ned as a birth weight < 2500 g. Very low birth weight (VLBW) is defi ned as a birth weight < 1500 g. Preterm delivery (PTD) was defi ned as delivery before 37 completed weeks of gestation. Fertility problems were defi ned as failure to conceive during a 1-year period, or longer, of regular contraceptive-free intercourse.
Tests and investigations
Chromosomal abnormalities Signifi cant rearrangements (e.g., balanced translocations such as reciprocal or Robertsonian) detected in peripheral blood analysis. Abnormalities in either the woman or her partner were considered positive. Uterine anatomic defects were identifi ed by hysteroscopy or 3-D ultrasound. Considered abnormal were: congenital uterine anomalies (such as septum, and unicornuate and bicornuate uteri), fi broids and polyps > 1.0 cm in the cavity, and Asherman ’ s syndrome adhesions.
Autoimmune disorders Lupus anticoagulant : Serum levels of lupus anticoagulant were evaluated using the dilute Russell viper venom test and PTT-LA. Results longer than 42 s, which were not corrected with a 1:1 mix of normal serum, were considered abnormal if confi rmed by a hexagonal phase phospholipid test.
Anticardiolipin antibodies Serum levels of anticardiolipin IgG and IgM were measured by enzyme-linked immunoassay, with abnormal levels exceeding 15 phospholipid units. All positive tests were confi rmed by repeat testing at least 12 weeks later.
Factor V Leiden mutation This category was considered abnormal if a heterozygous or homozygous factor V Leiden G1691A mutation was found.
Other non-APL thrombophilias Heterozygous or homozygous mutations for the G20210A prothrombin (factor II) gene were considered abnormal.
Thrombophilic factors Serum levels of functional protein C activity < 70 % , functional protein S activity < 70 % , or antithrombin activity < 75 % were considered abnormal. Each thrombophilic factor was analyzed independently.
Thyroid function TSH serum levels < 0.45 mU/mL or > 4.5 mU/mL were considered abnormal.
Antithyroid peroxidase and antithyroid antibody Positive result was considered abnormal.
Blood glucose level A patient ’ s serum glucose level was considered abnormal if fasting blood glucose was > 126 mg/dL.
Prolactin Serum levels of prolactin (PRL) > 23 ng/mL were considered abnormal.
Anti nuclear antibody (ANA) Positive result was considered abnormal.
Rheumatoid factor(RF) Positive result was considered abnormal.
Statistical analysis
Statistical analysis was conducted using SPSS software (version 17.0; SPSS Inc., Chicago, IL, USA). Frequencies were compared by the χ 2 -test and Fisher ’ s exact test and by means of continuous data by t -test. Multivariable logistic regression analysis was used to determine the role of primary vs. secondary RPL in the incidence of preterm delivery at the index pregnancy, controlling for risk factors that were found in the univariate analysis to be associated with primary RPL.
Results
Table 1 presents the socio-demographic and medical characteristics of the two study groups. Among 716 patients admitted to the RPL clinic during the study period, 420 met the inclusion criteria; 162 (38.6 % ) women were classifi ed as primary and 258 (61.4 % ) as secondary RPL.

The length of surveillance time was similar in both study groups. The mean maternal age at evaluation and proportion of women with previous surgeries were signifi cantly higher in the secondary RPL group than the primary RPL group. The rate of smokers was slightly higher (statistically insignifi cant) among the secondary RPL group than in the primary RPL group. There were no alcohol users among the subjects. None of the other demographic or obstetric characteristics were signifi cantly different between the two study groups.
Table 2 presents pre-index pregnancy characteristics. The mean number of miscarriages pre-index was signifi cantly lower in the primary RPL group than in the secondary RPL group (3.1 ± 1.4 vs. 3.6 ± 1.6, P < 0.001). In the primary RPL group, the majority of women had two or three miscarriages, while the majority of women in the secondary RPL group had three or four or more miscarriages. No differences were observed in timing (week of gestation) of the previous two miscarriages.

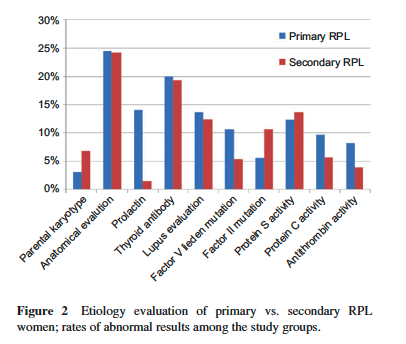
Table 3 describes the diagnostic tests performed during evaluation. There was no difference in the proportion of women who had undergone the minimal set of tests (defi ned as: parental karyotype, anatomic evaluation of the reproductive tract, lupus anticoagulant, and anticardiolipin IgG and IgM). A signifi cant difference was found only in prolactin levels; a higher rate of abnormal results was found in the primary RPL group than in the secondary RPL group (14.1 and 1.4 % , respectively, P < 0.001). Most of these women had mild hyperprolactinemia (data not shown). Fasting glucose levels for all women tested were within the normal range; 152 primary RPL women and 247 secondary RPL women (not including 10 primary and 11 secondary RPL women who were not tested).
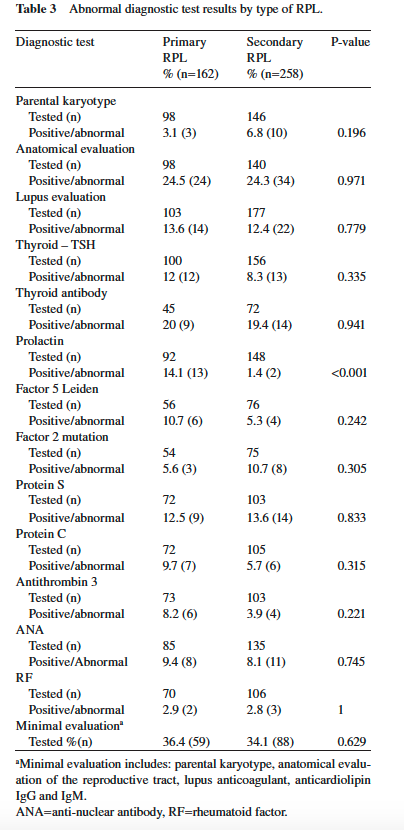
At least one abnormal test result was found in 43.8 % of the primary RPL group and 40.7 % of the secondary RPL group; this difference was statistically insignifi cant (P = 0.527).

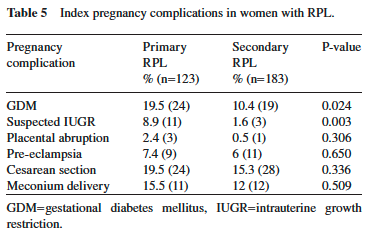
Table 4 describes the index pregnancy characteristics and outcomes and Table 5 presents the index pregnancy complications. The mean maternal age of the secondary RPL group at the time of index pregnancy was signifi cantly higher than that of the primary RPL group. The live birth rate was similar between the two groups (75.9 % in the primary RPL group vs. 70.9 % in the secondary RPL group). The mean gestational age at the time of delivery was signifi cantly lower in the primary RPL group than in the secondary RPL group, and the rate of preterm births was signifi cantly higher in the primary RPL group.
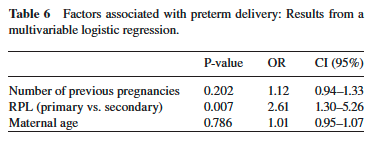
The majority of miscarriages occurred at 6 – 10 weeks after gestation in both groups. In addition, a signifi cantly higher rate of fertility problems was found in the primary RPL group compared with the secondary RPL group Table 6 Factors associated with preterm delivery: Results from a multivariable logistic regression. P-value OR CI (95 % ) Number of previous pregnancies 0.202 1.12 0.94 – 1.33 RPL (primary vs. secondary) 0.007 2.61 1.30 – 5.26 Maternal age 0.786 1.01 0.95 – 1.07 (13 vs. 5.8 % , P = 0.011). We found signifi cantly higher rates of PTD, GDM, SGA and LGA in the primary RPL compared to the secondary RPL group. In order to examine the independent risk factors for PTD associated with primary vs. secondary RPL, we conducted a multivariable logistic regression analysis adjusting for possible confounders. Variables that were found to be signifi cant in the univariate analysis were included in the model. Adjusting for maternal age and gravidity, primary RPL compared with secondary RPL was found to be an independent risk factor for preterm delivery (2.6 × increased risk; Table 6 ).
Discussion
The main purpose of this cohort study was to determine the risk factors and prognoses of women with a history of two or more consecutive pregnancy losses without any live births and those of women who had at least one live birth.
The most important fi nding of the study was that the rate of successful index pregnancy was similar between these two groups of women with RPL. Our fi ndings strengthen what has been previously reported by Clifford et al., however, a previous live birth conferred no advantage to the outcome of the next pregnancy, on the likelihood of a live birth in the subsequent pregnancy in women with RPL [7] . Brigham et al. reported no signifi cant difference between these two groups, and added that women with a history of two previous miscarriages had similar chances of success in a subsequent pregnancy to those who had three (76 vs. 79 % ) [5] . However, Alberman reported that the risk of another miscarriage after a series of consecutive losses increases signifi cantly for primary RPL women [1] . This inconsistency may be explained by different study groups and populations. A number of socio-demographic and medical characteristics of women who attended the RPL clinic in Soroka University Medical Center have been collected (presented in Tables 1 and 2) in order to examine whether there are major differences between the groups and predisposing factors for the next pregnancy outcome.
Our study population comprised 39 % primary RPL and 61 % secondary RPL women in contrast to recent studies that reported different proportions (the primary RPL group constitutes about 60 % and secondary RPL about 40 % [14, 16] . This was unexpected, since it was assumed that women with a child (or children) would be less likely to be referred to an RPL clinic than women without any successful pregnancy. The cultural characteristics of the study population (especially Bedouins) and the high value placed on fertility, can provide a possible explanation, and may cause women to seek treatment regardless of the number of children they already have. Additionally, there may be a lower prevalence of primary compared to secondary RPL women in our population; however, we are not able to evaluate accurate rates in our general population.
As expected, mean maternal age was higher among secondary RPL women, probably because of the greater gravidity (Table 2). The signifi cant difference between the groups in the rate of previous surgeries can be attributed to the higher rate of gynecologic surgeries (including deliveries by cesarean sections that the secondary RPL women underwent in their previous births). About 60 % of the pregnancy losses among the two groups occurred during 6 – 10 weeks of gestation. This fi nding was consistent in all pregnancy losses we have recorded. This supports previous fi ndings demonstrated by Heuser et al., regarding women with idiopathic RPL who tend to have losses recur at the same gestational age period [12] .
A considerable number of studies have been conducted to evaluate the etiology of RPL; however, only a few compared primary with secondary RPL [14] . We found that the only signifi cant difference between the groups after etiology evaluation was in prolactin levels. The prevalence of abnormal results was 10 times greater among primary RPL woman (14.1 % ) compared to secondary RPL woman (1.4 % ). The prevalence of hyperprolactinemia ranged from 0.4 % in an unselected normal adult population to as high as 9 – 17 % in women with reproductive disorders [4] . The higher rate of abnormal prolactin levels might explain the signifi cantly higher rate of fertility problems found in the primary RPL group compared to the secondary RPL group (13 vs. 5.8 % , respectively).
The results of the thrombophilic workup were not statistically different between the two groups; however, there was a tendency for most of the thrombophilias to occur among the primary RPL women (Figure 2 ). Accordingly, a signifi cantly higher rate of thromboprophylaxis was given during the index pregnancy to women with primary RPL compared to women with secondary RPL (32.7 vs. 22.5 % ).
The rate of unexplained etiology for RPL, as described in previous studies, is around 50 – 60 % [10, 14, 23] . Our fi ndings are consistent with the literature in this respect. Furthermore, at least one abnormal test result was found among 43.8 % of the primary RPL group and 40.7 % of the secondary RPL group, which leaves the remaining cases unexplained/unknown after evaluation. It should be noted that only 35 % of the total group had a minimal evaluation, so this emphasizes the need to continue the investigation in women with an unknown cause of RPL and at the same time, give supportive care and close surveillance, to decrease as much as possible maternal stress, as this mode of intervention has been shown to signifi cantly improve the pregnancy outcome [7] .
While the association between RPL and adverse obstetric and neonatal outcomes has been well established in the literature [3, 16, 18, 23, 25] , little attention has been given to the type of RPL. Only two studies compared primary with secondary RPL. Jivraj et al. [16] investigated the pregnancy complications in 162 women with three or more recurrent miscarriages, and found higher rates of gestational hypertension (8.4 vs. 6 % ) and preterm delivery (18 vs.7.7 % ) among women with primary compared with secondary RPL; however, no adjustment was made for maternal age and parity. Nielsen et al. [18] compared obstetric and neonatal complications of preceding pregnancies in secondary RPL and nulliparous women, and found that they were frequent and appeared to be associated with an increased risk of complications in on-going pregnancies following the secondary RPL diagnosis. The study did not compare the results to those of primary RPL women.
We found significantly higher rates of obstetric and neonatal complications among the primary compared with the secondary RPL group, including preterm delivery, low birth weight, small for gestational age, large for gestational age, and gestational diabetes mellitus (Tables 4 and 5). The crude rates of preterm delivery and low birth weight in the secondary RPL group were similar to the unadjusted rates presented by Jivraj et al. and Nielsen et al. In order to adjust for potential confounders, multivariable logistic regression analysis has been conducted. Primary RPL was found to be an independent risk factor for PTD compared to secondary RPL (2.6 × increased risk) adjusted for maternal age and gravidity. Increasing number of previous pregnancies and maternal age were not found to be independent risk factors. We found a signifi cant increase in odds of PTD with an increasing number of previous miscarriages (OR 1.34, CI (95 % ) 1.07 – 1.69; data not shown). This fi nding is in line with what has been reported in previous studies [3, 16, 23] . The risk of preterm delivery generally appears to be greater in women with recurrent miscarriage in comparison with the general population. According to Hammoud et al., in nulliparous women, the risk for preterm delivery increased exponentially with an increasing number of previous miscarriages [11] . Brown et al. also found that the risk for low birth weight and preterm delivery increases with an increasing number of previous miscarriages [6] . However, we think that the reproductive performance (gravidity) should be taken into consideration when comparing primary with secondary RPL women. Additionally, we detected signifi cantly higher levels of GDM among the primary RPL group compared with the secondary (19.5 and 10.4 % , respectively). Previous studies have reported increased rates of impaired glucose tolerance in women with RPL [13, 23] . However, there was no focus on this study ’ s subgroups. The difference we found between the groups may be associated with the higher rates of other complications in the index pregnancy found among the primary RPL group, such as LGA, PTD, and hyperprolactinemia (possibly as a part of polycystic ovary syndrome).
In conclusion, this cohort study focused on two important RPL subgroups that have not been suffi ciently researched. The comparison between these two groups of women is essential in order to correctly evaluate the prognosis and thereby offer the best consultation and follow-up. We found that having a live births prior to two or more RPLs, does not affect the likelihood of a subsequent successful pregnancy. In agreement with other studies, our study shows an increased risk for adverse obstetric outcome such as preterm delivery, fetal growth restriction, and gestational diabetes mellitus. The increased risk of PTD associated with primary RPL persists after controlling for age and gravidity, suggesting that women with primary RPL are more prone to complications than women with secondary RPL. Therefore, we recommend careful surveillance, especially of primary RPL women, for the detection of complications as early as possible.
Study limitations
The main weaknesses of the study are that it is retrospective and contains a relatively small number of women. However, since our medical center is a tertiary hospital, the RPL clinic receives most of the patients from the area, so it refl ects the local population. Additionally, we believe that this problem should be further investigated and results should be compared to general obstetric populations as a control group.
References
[1] Alberman E. The epidemiology of repeated abortion. In: Beard RW, Sharp F, editors. Early pregnancy loss: mechanism and treatment. London: Royal College of Obstetrics and Gynaecology Press; 1988. pp. 9 – 17.
[2] American College of Obstetricians and Gynecologists (ACOG). Management of recurrent early pregnancy loss. ACOG practice bulletin. Int J Gynaecol Obstet. 2002;78: 179 – 90.
[3] Bhattacharya S, Townend J, Bhattacharya S. Recurrent miscarriage: Are three miscarriages one too many ? Analysis of a Scottish population-based database of 151,021 pregnancies. Eur J Obstet Gyn R B. 2010;150:24 – 7.
[4] Biller BMK, Luciano A, Crosignani PG, Molitch M, Olive D, Rebar R, et al. Guidelines for the diagnosis and treatment of hyperprolactinemia. J Reprod Med. 1999;44:1075 – 84.
[5] Brigham SA, Conlon C, Farquharson RG. A longitudinal study of pregnancy outcome following idiopathic recurrent miscarriage. Hum Reprod. 1999;14:2868 – 71.
[6] Brown JS Jr, Adera T, Masho SW. Previous abortion and the risk of low birth weight and preterm births. J Epidemiol Commun H. 2008;62:16 – 22.
[7] Clifford K, Rai R, Regan L. Future pregnancy outcome in unexplained recurrent fi rst trimester miscarriage. Hum Reprod. 1997;12:387 – 9.
[8] Defi nitions of infertility and recurrent pregnancy loss. Fertil Steril. 2008;89:1603.
[9] Dollberg S, Haklai Z, Mimouni FB, Gorfein I, Gordon ES. Birth weight standards in the live-born population in Israel. Israel Med Assoc J. 2005;7:311 – 4.
[10] Ford HB, Schust DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev Obstet Gynecol. 2009;2:76 – 83.
[11] Hammoud AO, Merhi ZO, Diamond M, Baumann P. Recurrent pregnancy loss and obstetric outcome. Int J Gynecol Obstet. 2007;96:28 – 9.
[12] Heuser C, Dalton J, Macpherson C, Branch DW, Porter TF, Silver RM. Idiopathic recurrent pregnancy loss recurs at similar gestational ages. Am J Obstet Gynecol. 2010;203:343. e1 – 5.
[13] Hughes N, Hamilton E, Tulandi T. Obstetric outcome in women after multiple spontaneous abortions. J Reprod Med. 1991;3:165 – 6.
[14] Jaslow CR, Carney JL, Kutteh WH. Diagnostic factors identifi ed in 1020 women with two versus three or more recurrent pregnancy losses. Fertil Steril. 2010;93:1234 – 43.
[15] Jauniaux E, Farquharson RG, Christiansen OB, Exalto N. Evidence-based guidelines for the investigation and medical treatment of recurrent miscarriage. Human Hum Reprod. 2006;21:2216 – 22.
[16] Jivraj S, Anstie B, Cheong YC, Fairlie FM, Laird SM, Li TC. Obstetric and neonatal outcome in women with a history of recurrent miscarriage: a cohort study. Hum Reprod. 2001;16: 102 – 6.
[17] Macklon NS, Geraedts JP, Fauser BCJM. Conception to ongoing pregnancy: the “ black box ” of early pregnancy loss. Hum Reprod Update. 2002;8:333 – 43.
[18] Nielsen HS, Steffensen R, Lund M, Egestad L, Mortensen LH, Andersen A-MN, et al. Frequency and impact of obstetric complications prior and subsequent to unexplained secondary recurrent miscarriage. Hum Reprod. 2010;25:1543 – 52.
[19] Rai R, Regan L. Recurrent miscarriage. Lancet. 2006;368: 601 – 11.
[20] Regan L, Braude PR, Trembath PL. Infl uence of past reproductive performance on risk of spontaneous abortions. Br Med J. 1989;299: 541 – 5.
[21] Stephenson M, Kutteh WH. Evaluation and management of recurrent early pregnancy loss. Clin Obstet Gynecol. 2007;50:132 – 45.
[22] Stirrat GM. Recurrent miscarriage I: defi nition and epidemiology. Lancet. 1990;336:673 – 5.
[23] Tulppala M, Palosuo T, Ramsay T, Miettinen A, Salonen R, Ylikorkala O. A prospective study of 63 couples with a history of recurrent spontaneous abortion: contributing factors and outcome of subsequent pregnancies. Hum Reprod. 1993;8:764 – 70.
[24] Van den Boogaard E, Kaandrop SP, Franssen MTM, Mol BWJ, Leschot NJ, Wouters CH, et al. Consecutive or non-consecutive recurrent miscarriage: is there any difference in carrier status. Hum Reprod. 2010;25:1411 – 4.
[25] Yang CJ, Stone P, Stewart AW. The epidemiology of recurrent miscarriage: A descriptive study of 1214 prepregnant women with recurrent miscarriage. Aust NZ J Obstet Gyn. 2006;46:316 – 22.
The authors stated that there are no confl icts of interest regarding the publication of this article.
Received December 30, 2011. Accepted January 25, 2012. Previously published online February 29, 2012.

